Reporting Highlights
- Treated as a Liability: Emily Waldorf was denied care for a risky miscarriage due to Arkansas’ abortion ban, even after she met the hospital’s CEO, called the governor’s office and got a lawyer.
- Lawyers, Not Doctors: Medical standards say it’s necessary for doctors to offer abortion. Women have died without it. But in states with bans, lawyers often decide if patients get care.
- An Isolated Fix: Texas recently provided guidance that says doctors don’t need to wait for miscarrying patients to get sicker before intervening. Arkansas and other states have not.
These highlights were written by the reporters and editors who worked on this story.
On the morning of Sept. 16, 2024, Emily Waldorf’s preschooler found her curled on the bathroom floor. Waldorf had felt a strange pressure during a shower, like a balloon bulging into her vagina, and was now bleeding. “I can be your pillow, mommy,” her daughter said, nuzzling into her neck.
Waldorf was 17 weeks pregnant. She and her husband, Justin, dropped their daughter off at her grandparents’ and rushed to Washington Regional Hospital in Fayetteville, Arkansas, where Waldorf worked as an acute care physical therapist.
In a dark room, a doctor pointed to an hourglass shape glowing on the ultrasound screen: There was her amniotic sac, funneling into her dilated cervix, and there was their tiny daughter’s foot, dipping out.
“Your body is about to miscarry,” the doctor said.
Three doctors gathered and told the couple that the longer Waldorf’s cervix remained open and her uterus exposed to bacteria, the higher her risk of developing a life-threatening infection. The standard of care, they explained, would be to quickly empty her womb.
But they couldn’t do that, one doctor said apologetically, sighing deeply. The baby still had a detectable heartbeat, and stopping it would run afoul of a state abortion ban that snapped into place after the Supreme Court overturned Roe v. Wade in 2022; violations carried penalties of up to $100,000 in fines and 10 years in prison. They needed to wait until Waldorf went into labor on her own or showed signs of a dangerous infection, or until the fetal heartbeat ended.
“Our hands are tied behind our backs,” Dr. Erin Large later told her, according to a journal Waldorf began keeping on her phone and shared with ProPublica. “Tell your friends to vote differently.”
Raised Baptist in a Republican family, Waldorf struggled to understand what the doctors were saying as waves of grief hit her. How could an abortion ban aimed at women who wanted to end their pregnancies keep doctors from helping a woman who didn’t?
Waldorf didn’t oppose abortion, but she had never considered that the law could apply to her. Her father was a doctor. This was the hospital where she had worked for the past six years. The OB-GYN team treating her had delivered her daughter, and some of them lived blocks from her parents. She was a highly educated 38-year-old woman with connections to the governor. As she lay in a hospital bed, worried that infection could enter her uterus at any moment, she finally understood the ban now applied to anyone losing a baby.
Trapped in a medical limbo, she took a nurse friend’s advice and began writing everything down. That journal, along with her medical records and interviews, offer a rare, harrowing account of how Arkansas’ abortion ban, not best practices or medical training, guided her doctors’ choices.
She was miscarrying as hospitals, physicians, lawmakers and medical boards around the country were being confronted with the reality that the bans, designed to be as strict and punitive as possible, were causing preventable harm and even deaths. Yet even as more of these cases stacked up, there was no coordination between states to protect women. Each state, each woman seemed to operate in a vacuum. And Waldorf would find she was in it alone.
One of the doctors advised Waldorf to go home and told her what to expect: At any moment, she could start bleeding heavily and go into labor. It might happen while she was going to the bathroom or playing on the floor with her daughter.
When the baby started to emerge, the doctor said, Waldorf shouldn’t pull too hard or she could rip the baby’s head off. She would need to cut the umbilical cord herself and return to the hospital for care in a diaper, her fetus wrapped in towels and the cord hanging between her legs.
Waldorf didn’t want her daughter, or herself, to have those memories inside their home. So she begged to stay, and the doctors agreed. No one could predict when the ordeal would be over.
Waldorf settled into a small hospital room, her husband glued to the vinyl couch beside her, both reeling from the impending loss of what would have been their second daughter.
The pregnancy had been far enough along to start getting their 4-year-old daughter excited about decorating a nursery, family-of-four camping trips and what it would mean to become a big sister.
Now they had to engage in the morbid ritual of waiting for that dream to die. Doctors and nurses with Doppler machines and ultrasounds kept showing up, forcing them to hear the heartbeat and see the movement of a tiny body. “Oh look,” Large said during one of the ultrasounds, “she’s opening and closing her mouth.”
“My body failed a baby,” Waldorf wrote in her journal.
Waldorf’s job, treating critical patients in the intensive care unit, had taught her to compartmentalize, to stay cool under pressure. But as the days bled together, her resolve turned to panic when she discovered one outcome she had not considered.
Scrolling through social media on her third night, a headline caught her eye: “Abortion Bans Have Delayed Emergency Medical Care. In Georgia, Experts Say This Mother’s Death Was Preventable.”
On the day Waldorf was admitted to the hospital, ProPublica had published an investigation on the death of Amber Thurman, a 28-year-old medical assistant who died of infection after doctors delayed emptying her uterus. Thurman left behind a 6-year-old son.
“Oh my god, it isn’t just me,”Waldorf thought.“But she died.”

Almost exactly three years before Waldorf showed up at Washington Regional in urgent need of care, a 28-year-old woman named Josseli Barnica arrived at a Houston emergency room with the same condition. She, too, was 17 weeks pregnant. The fetus’ head was pressed up against her dilated cervix, and a miscarriage was, according to her medical record, “inevitable.”
When her husband rushed from work to her side, she relayed what she said the medical team had told her: Inducing delivery or emptying her uterus would be “a crime,” he later told ProPublica. “They had to wait until there was no heartbeat.”
Texas, like Arkansas, has a criminal abortion ban. Had Barnica landed in one of the hospitals across the world, from Nigeria to Mexico, that follow standards from the World Health Organization and countless medical associations, her treatment would have been much different.
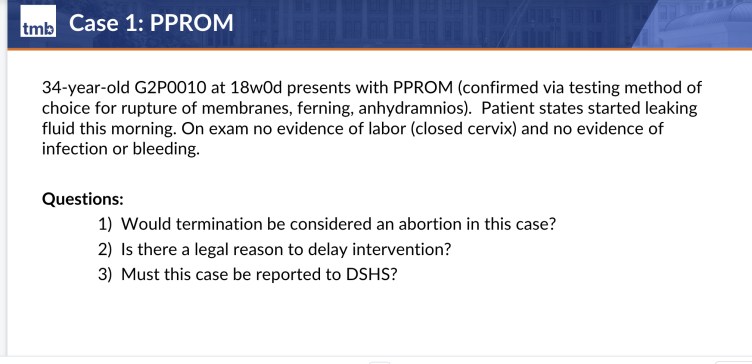
In those hospitals, when a patient’s cervix opens too soon, signaling an “inevitable miscarriage,” or when their water breaks before the fetus can survive, known as previable preterm premature rupture of membranes (shorthanded as “PPROM”), it’s standard for doctors to offer to empty the uterus. That’s true even if there is still a heartbeat, given the high risk of infection.
“This is basic obstetrics,” said Dr. Alison Goulding, a maternal-fetal-medicine specialist in Texas. “Everyone should know that you have to provide an abortion in these settings or women can die.”
For 40 hours, Barnica waited in the hospital for the heartbeat to stop, with her cervix exposed to bacteria. She died three days after she delivered, ProPublica reported in October 2024; the cause was a deadly infection. The hospital declined to comment on Barnica’s case but said “our responsibility is to be in compliance with applicable state and federal laws and regulations” and physicians exercise their independent judgment. The doctors involved did not respond to requests for comment.
Her death and those of six other women in three states over the next three years brought into sharp focus the consequences of the bans. Because the laws’ exceptions for medical emergencies are vague and have rarely been tested in courts, liability-conscious hospital administrators, lawyers and doctors have sometimes put legal concerns above their patients’ well-being, ProPublica’s reporting has found.
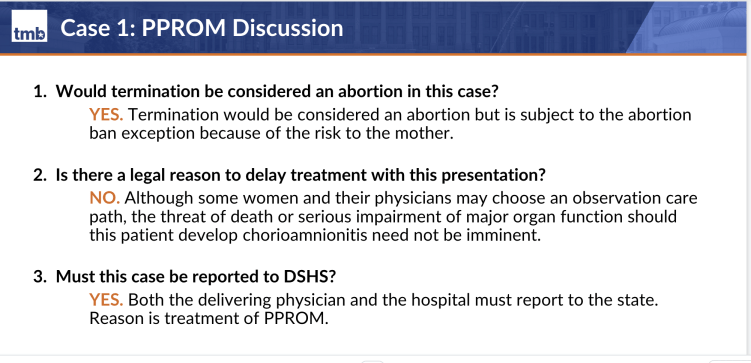
Texas lawmakers responded to ProPublica’s investigations by amending the exceptions in their state laws to make clear that a life-threatening emergency did not need to be “imminent” for physicians to act. The state’s medical board specified that doctors can empty the uterus of any patient with PPROM, and it requires doctors to undergo training to ensure they know that.
But Texas’ reforms stopped at its borders. Without a single federal law governing abortion, each of the 19 other states with similar bans were not required or advised to follow suit. That includes Arkansas, which touts its designation as the “most pro-life state in America.”
Since its ban took effect, not one person there has been granted a medically necessary abortion, according to the state’s public data.
The state’s Republican lawmakers and officials have repeatedly shot down attempts to broaden the law’s exceptions. And when advocates tried to launch a ballot initiative to let voters weigh in, Republicans blocked it over a paperwork error and created restrictions to make those initiatives harder to file.
The doctors and Democrats fighting for reform have been doing so without essential knowledge that could help make their case. Though the two states share a border, news of Texas’ changes to its abortion ban — and why they were made — had failed to have an impact across the state line.
Three Democratic state representatives said they hadn’t heard of the new Texas guidance until ProPublica asked about it. “If there are things that are working in other states, we should be looking at that,” said one, Ashley Hudson, who has tried twice to pass broader exceptions.
On her fourth morning in the hospital, Waldorf was sitting on the toilet when she felt something heavy fall. There was so much blood, she couldn’t see what it was. She thought it was the baby, but a nurse confirmed it was a blood clot, 3 inches across.
Waldorf’s water had broken. All morning, she watched the amniotic fluid drain out of her. Now there was virtually no chance the fetus’s lungs would develop to reach the edge of viability in seven weeks. There was only the risk of infection, growing every passing hour.
She was convinced that this meant the doctors would finally have to induce her to avoid infection. But after confirming that her fetus still had heart tones, the OB-GYN on duty, Dr. Britte Smith, said she couldn’t induce yet. First she’d need to consult the hospital’s risk-management team.
“Oh,” Waldorf thought. “I’m a liability.”
Smith returned about two hours later, Waldorf recalled, and told her she had two options: She could remain under observation at the hospital, or she could get into her car and drive nearly four hours to Kansas, a state with no abortion ban, where doctors could induce her. The hospital would not authorize a transfer or arrange to send her in an ambulance, and it offered no explanation for why.
Medical records note that the risk-management team was consulted twice over the next 31 hours, and Smith wrote: “Since there is still a heartbeat and no signs of maternal infection, we can not proceed” with induction of labor. Smith did not respond to requests for comment.
Waldorf called the maternal-fetal-medicine team at the University of Arkansas for Medical Science in Little Rock, the state’s only academic health center. The team told her standard treatment guidelines recommended that she be induced if she didn’t deliver within 12 to 24 hours because the risk for infection rises every hour. But they also said: “It can’t be done in Arkansas.” The hospital told ProPublica it could not comment on Waldorf’s experience.
Waldorf’s sister, Elizabeth Rowe, had almost died of hemorrhaging during childbirth, so the family felt an hourslong drive to Kansas through rural roads without medical support was not an option.
Waldorf’s family and friends were shocked she was running into so many obstacles. Her father, a gastroenterologist named Kenneth Rodgers, was baffled. “You don’t sit around and wait for somebody to become septic. You do whatever it takes to prevent them from becoming septic,” he said. “If I don’t do what’s medically indicated in a potentially life-threatening situation, then I am liable for neglect. Why isn’t this the same thing?”
Her mother and stepfather were also outraged.
“It’s inhumane,” her mother, Linda Quattlebaum, said. “I’m pro-life, but for the mother.” Her husband, Paul Quattlebaum, fumed, “If I took my dog to a vet and it had this problem, that dog would get better treatment.”
The next morning, day five, 24 hours had gone by since Waldorf’s water broke. She texted a friend from college that her temperature had risen to 99.3 degrees.
“What is next?” her friend, Lindsey Haire, wrote back. “Can they help you now?”
“I think it has to be like 100.4,” Waldorf wrote. “They will continue to monitor my temp or my symptoms.”
“Dear lord,” Haire responded.
Waldorf had spelled out the catch-22 in her journal that morning: “If I need a blood transfusion and it stabilizes my condition, they cannot induce. If my temp continues to spike then they can induce.”
When her sister, Rowe, walked in that morning, she found Waldorf with her eyes wide and glazed over, her jaw tensed. Justin slumped on the couch looking defeated. “Are they going to let me die?” Waldorf asked.
Rowe had never seen her sister this way; Waldorf was always the calm and practical one when challenges arose.
“That’s crazy,” Rowe said. “We’re in a hospital. People come to the hospital for them to save your life, not to let you die.”

Some hospitals in states with abortion bans have taken steps to protect their patients.
When Ohio was under a six-week ban in 2022 and 2023, a group of hospitals in one region gathered to hash out collective policies, including for miscarriages, said Dr. Justin Lappen, the chair of the Society for Maternal Fetal Medicine’s committee on reproductive health. “Everyone at the same time thought the worst thing to do would be to have different practices,” he said.
So they resolved to interpret the vague law the same way: PPROM qualified as a medical emergency. “There’s power in numbers,” he said. “If we are going to do something, we should do it together and be similar, because that also hopefully gives you legal protection.”
But that’s far from the norm. A 2024 Senate Finance Committee report, commissioned in the wake of ProPublica’s reporting on Thurman’s death, found that many hospital leaders and lawyers have left doctors to fend for themselves and have at times remained “conspicuously and deliberately silent” on how to provide care for miscarriages under the bans.
Physicians described hospital lawyers who “refused to meet” with them for months, were “pretty much impossible” to reach during “life or death” scenarios, and offered little help beyond “regurgitating” the law, according to the report. Information on how to handle the legal conflicts between the bans and federal law is usually not written down and, in some cases, is provided only on a “need-to-know” basis.
ProPublica has also reported that hospitals in different regions of Texas took vastly different approaches to treating miscarriage — and that miscarrying patients were far more likely to get gravely ill where hospitals weren’t offering abortions without signs of infection.
Many hospitals in abortion ban states will not even disclose their policy on PPROM to the public, ProPublica surveys have found. Of 10 hospitals with significant labor and delivery wards in Arkansas, only one responded to ProPublica’s questions.
The University of Arkansas Medical Sciences shared its frequently asked questions on abortion policy that stated, in part, “Under Arkansas law, may an abortion be performed if the mother’s life is at risk? It depends.” Only abortions “necessary” to preserve a patient’s life are allowed, not ones that could prevent “possible” emergencies, according to the hospital’s general counsel.
“Hospital leaders and institutional lawyers are basically interpreting these laws so conservatively, and so worried about a criminal charge, that they have forgotten about basic professionalism values of healthcare,” said Dr. Jody Steinauer, a professor of OB-GYN at the University of California, San Francisco who studies the impacts of abortion bans.
In interviews with seven doctors who worked in Arkansas, all said that no hospitals allow doctors to provide abortions for patients with “inevitable miscarriage” or PPROM without signs of infection.
Dr. Dina Epstein, an OB-GYN in Little Rock, said she and her colleagues see cases like Waldorf’s often. They are always excruciating.
Her patients often panic and beg for help, but none have had the resources to travel to another state for care. Doctors at her hospital are left to negotiate among themselves over what counts as sick enough for them to act, Epstein said. “What organ needs to fail? What thing needs to happen that pushes us over the edge?”
Many hospitals and doctors remain paralyzed, experts say, even though none have been prosecuted for treating a miscarriage with a procedure that would be considered an abortion.
“It’s been five years, and people are still like: ‘I don’t know what we can do,’” said Ghazaleh Moayedi, a doctor in Texas who never stopped providing abortions for women facing miscarriages. “That’s willful ignorance at this point.”
Rowe wracked her brain for something, or someone, who might be able to help her sister.
She began calling up private ambulance companies, but they would not agree to drive Waldorf because they considered her condition unstable. The cost of a medevac helicopter was in the tens of thousands of dollars. Rowe considered putting it on a credit card.
Then it struck her. “Let’s call up Sarah,” Rowe said.
The family didn’t personally know Gov. Sarah Huckabee Sanders, but in their small-town Baptist circles, she felt only a degree away. Waldorf had gone to the same college, four years behind, and joined the same sorority, known as a social club, at Ouachita Baptist University. They had friends whose cousins had been in the governor’s wedding or had gone on vacation with her. One of those friends had even invited Waldorf to stay at a historic eight-room bed and breakfast with the governor during Ouachita’s annual alumni event in two weeks’ time.
On Waldorf’s fifth day in the hospital, Rowe reached an aide in the governor’s office at 9:27 a.m., according to Waldorf’s journal. She tried to lay it on thick, telling the aide about the connections Waldorf and Sanders shared.
“We recommend you seek legal advice,” the aide responded.
“This is an emergency,” Rowe countered. “We need some help now!”
The aide’s reply, according to Rowe: “What is it you expect the governor’s office to do?”
The sisters had the law’s exception language pulled up on a phone. It defined a medical emergency as “a condition in which an abortion is necessary to preserve the life of a pregnant woman whose life is endangered by … a physical condition caused by or arising from the pregnancy itself.” Waldorf’s case certainly counted, they argued, and they begged for someone to call the hospital and the attorney general’s office.
The aide offered to learn more and call back, but the family says it never received another call. A friend also called the governor’s office twice and reached two different aides and got a similar response. ProPublica asked the governor’s office if Sanders was aware of the calls at the time, and if not, what her message would be to women facing this kind of situation. The spokesperson did not respond to the questions, but said: “Governor Sanders has prioritized not just the wellbeing of Arkansas’ unborn children but also at-risk kids and mothers.”
A friend reached out to Molly Duane, at the time a senior attorney at the Center for Reproductive Rights, who was representing dozens of women denied medical care under abortion bans. Among them was Amanda Zurawski, a Texas woman who contracted sepsis and lost a fallopian tube in 2021 after doctors refused to induce her at 18 weeks pregnant in circumstances much like Waldorf’s. In response to that case, the Texas Supreme Court said PPROM should count as a medical emergency.
When Duane received the call, she was confident she had the expertise and the data to fix any fear or misunderstanding the hospital might have. “This is not a hospital in the middle of nowhere,” Duane said, “This is the hospital where she works. Surely I can convince them that providing the standard of care is legal.”
Her arguments made little headway. In a conversation with Andrew Cozart, the hospital’s director of risk management, and Thomas Olmstead, its general counsel, Olmstead told her, “We cannot rule out the possibility of an overzealous prosecutor,” she recalled.
Duane sent Cozart evidence it would be a violation of medical standards and common understandings of the law’s exception if the hospital didn’t provide Waldorf an induction. ProPublica reviewed the letter Duane sent and reached out to Cozart and Olmstead, who did not respond to requests for comment.
At 5 p.m., about an hour after the email was sent, Waldorf was getting out of the shower when the CEO of the hospital, Larry Shackelford, knocked on her door. “Let me put on some clothes first,” she told the nurse, flustered.
Waldorf was used to seeing Shackelford addressing staff at the front of a conference room, polished in a suit and tie. But when he opened the door, he looked disheveled, like he had stood up from his desk and run down the hall.
Waldorf and her husband recall him standing awkwardly at the foot of the bed as she looked at him with her arms crossed. “I feel like a ticking time bomb right now,” Waldorf told him. “I’ve been here for five days, and you guys have not done anything for me.”
“I’m so sorry you’re in this situation,” the Waldorfs recalled Shackelford saying. “We’re going to take the very best care of you.”
He didn’t say much else, except to repeat that she would get the best care, as if that was all he had been authorized to say. When he left, the couple was confused. Was Shackelford saying the hospital was finally going to allow an induction? Or was this a political visit meant to mollify them? Shackelford did not respond to a request for comment.
But Large returned and told them the hospital’s decision hadn’t changed. “With positive fetal heart rate and no evidence of maternal distress/severe illness at this time unable to augment/induce labor to expedite delivery,” the doctor wrote in the medical records; she advised they should consider going home.
Soon after, Washington Regional officials told Duane they would agree to transfer Waldorf to a hospital in Kansas, where abortion at her gestational stage was legal. Duane found a team at The University of Kansas Health System about four hours away.
Before authorizing the transfer, though, Large told Waldorf she had to say specific words.
“Repeat after me,” Large said, the Waldorfs and Rowe recall. “I no longer want to receive care here. I would like to transfer to another hospital with a higher level of care.”
Waldorf repeated the words, and they were noted in her medical record.
At 10:20 p.m., Waldorf was strapped into a five-point harness in the back of an ambulance and began the bumpy ride along rural roads. Her husband and sister followed behind, watching her anxiously through the window.
Her arrival at the Kansas hospital felt nothing like what she had experienced in Arkansas, Waldorf wrote. Women in green scrubs and hairnets were lined up to greet her as her stretcher rolled out of the elevator. Their leader, Dr. Megan Thomas, spoke first.
“We are so glad you made it,” she said.

The University of Kansas hospital system was not always this helpful.
Two years earlier, its legal team at a separate facility had blocked care to a woman named Mylissa Farmer for PPROM at 17 weeks, even though the state did not have a sweeping abortion ban.
The Biden administration investigated the case as a violation of the Emergency Medical Treatment and Labor Act, which it interpreted as dictating that hospitals must offer patients abortions in emergency situations, even if they are in states with bans.
Federal investigators learned that The University of Kansas Health System officials had deemed the political climate “too hot and heated” to help Farmer, according to their report. The government cited the hospital for violating the law and threatened fines if the system didn’t correct issues that led to the denial of care. The hospital said Farmer’s care was in line with hospital policy, medical standards and the law based on the facts known at the time. The University of Kansas Health System has since become something of a beacon for women in Waldorf’s situation.
It’s hard to see where that kind of accountability push would come from today.
The Trump administration rescinded the Biden-era guidance pressing hospitals to offer emergency abortions and dropped the government’s related lawsuit.
Republican lawmakers in states with bans haven’t introduced legislation to punish hospitals and physicians who fail to provide care, even though they often blame deaths and injuries under bans on malpractice and confusion.
And state medical boards, which oversee the licensure of doctors, have not disciplined physicians reported to have refused to perform a medically necessary abortion during a miscarriage, including the doctors involved in Barnica’s, Zurawski’s and Farmer’s care.
If the medical board in Arkansas could issue guidance about PPROM like the one put out in Texas, that would help enormously, doctors there told ProPublica. “It addresses the vagueness and all the specific questions we have as providers,” Epstein, the Little Rock doctor, said.
Even the prominent anti-abortion advocacy group Americans United for Life told ProPublica it agreed with the Texas stance on treating previable PPROM.
ProPublica asked the Arkansas Medical Board, the governor’s office and Republican lawmakers who sponsored the abortion ban if they planned to issue similar guidance.
The Arkansas board told ProPublica the law is already clear enough. Medical boards in 18 other states that banned abortion either said they did not have plans to issue new guidance or did not respond to ProPublica’s questions.
The governor’s office did not answer questions from ProPublica.
In response to ProPublica’s questions, Mary Bentley, a Republican state representative and lead sponsor of the original ban, said she believes that the law does allow doctors to offer abortions to women with PPROM and that they do not need to wait for signs of infection. She said she is reaching out to the medical board to see if they can issue guidance similar to Texas’ and she would work toward more legislation if needed.
“Medical decisions should not be made by lawyers,” she said. “We need to just clarify it for them better. The women of our state definitely deserve it.”
One of the last levers of accountability is the courts. Abortion-rights groups, including Amplify Legal, where Molly Duane is now the litigation director, have sued at least 13 states over their laws, sometimes forcing clarifying statements from judges — though they’ve had limited impact so far.
One lawyer in Texas has started filing malpractice lawsuits. Michelle Maloney represents 10 women or their families who allege doctors did not provide medical care that should have been considered legal under the abortion law’s medical emergency exception.
“I think it is the most effective way to potentially make hospital systems do what they need to do to support doctors,” Maloney said. “If we can create some risk on the other side, hopefully we can motivate people to do the right thing.”
Soon after Waldorf arrived at the Kansas hospital, she received misoprostol to induce labor and delivered around 1 p.m.
She and Justin held their daughter for a few precious moments as her heartbeat stilled, marveling at her perfect tiny fingers and toes and whispering private words of love.
They named her Bee, in honor of the interconnectedness of the natural world, and so they could see reminders of her each spring.
Then the tenor in the room turned. Waldorf’s placenta was having trouble detaching. Blood kept gushing out, soaking the pads under her dark red. The nurse kept weighing them.
“Is that a lot of blood?” Waldorf asked, her eyes locked with those of the nurse.
“It’s a lot of blood,” the nurse replied.
The monitor began beeping. Waldorf’s blood pressure was dangerously low. Justin saw his wife’s face turn white.
Working in the intensive care unit, Waldorf had seen patients die with this exact combination of symptoms. “This is it,” she thought.
A doctor reached elbow-deep into her uterus, trying to loosen the placenta. The team was about to take her to the operating room when he was finally able to detach it.
Doctors said she lost a liter of blood and her complications were likely worse for having been forced to wait so long to deliver.
Waldorf realized that if she had gone into labor at home or on the road, there was no way she would have made it to the hospital in time.
In Waldorf’s medical record, the Kansas doctors stated the induction was performed “with the intent to preserve the life and health of the mother.” It included four dense paragraphs citing evidence of the high risks of sepsis and hemorrhage if the medical team waited to empty her uterus.
Some hospitals in states with bans have provided similar prewritten language their physicians can use to remove ambiguity about why an abortion falls under an emergency exception. Washington Regional, which has not provided such guidance to its doctors, declined to comment on its policies. None of the doctors involved in Waldorf’s care at Washington Regional agreed to discuss the case.
Back at home, Waldorf’s mother came to stay. Waldorf continued to bleed so much that she didn’t want to go out in public and suffered headaches for a week. In her journal, she unpacked her grief and rage.
“It all feels quite like the Handmaid’s tale,” she wrote on Sept. 24. “I had to seek refuge, travel by ambulance across borders.”
She and Justin had a hard time explaining to their daughter what had happened when she would ask when her little sister would arrive. They told her she wasn’t coming anymore, until the girl eventually stopped asking.
Alumni weekend came around. Waldorf had canceled the stay at the bed-and-breakfast with the governor, but she decided seeing her community might be healing. At the opening event, the emcee announced that Sanders was in attendance and the audience rose to applaud. Waldorf stayed seated. So did her mother and stepfather, who had supported the governor for years.
Her stepfather tore the Sanders bumper sticker off his car and made it known to local politicians what had happened.
On Dec. 8, the night before she was scheduled to return to work, Waldorf found herself frantically cleaning her house and snapping at her daughter.
The next morning, she could barely push herself out of the car. Walking into Washington Regional, she was flooded with memories of the days she had spent there as a patient, and of how her colleagues and the CEO had not been able to help her.
A month later, she submitted her resignation letter. The decision made her feel lighter, she wrote. “Exhausted. Free.” She started her own physical therapy practice that spring, naming it Hive Therapy in honor of Bee.
She estimates the lost income, startup debt and out-of-pocket medical costs from her ordeal at more than $147,000. Included in the tally was more than $5,000 for the ambulance ride to Kansas, which Washington Regional was unwilling to pay for.
In a letter to Duane, the hospital’s general counsel, Thomas Olmstead, used Waldorf’s words against her — the words Large had asked her to repeat.
The ambulance transfer happened because of Waldorf’s “specific request,” he wrote, and not because the attending physician believed that Waldorf needed a “higher level of care.”
“It is simply not reasonable for you to make demand that WRMC assume responsibility for the cost of a patient-directed transfer,” he wrote. Olmstead has since been promoted to executive leadership. He did not respond to a request for comment.
When reached for comment, Large would not speak about Waldorf’s case even though Waldorf had given her permission to. But, she said, “I am glad that the topic at hand is being discussed, because that’s incredibly important. I’m glad her voice is being heard.”
The Arkansas Medical Board said it is not currently investigating any complaints against the doctors. Local lawyers have been unwilling to take on a malpractice case because Waldorf didn’t die or end up with permanent injuries.
A year after leaving her job, in February 2026, Waldorf joined a lawsuit led by Duane, alongside an OB-GYN and five other women denied care under the Arkansas abortion law. It seeks to block the state’s ban on the grounds that it violates the state constitution; named as defendants are Sanders, the Arkansas attorney general, state prosecutors and members of the state medical board. The state is currently trying to get the case thrown out on jurisdictional grounds, and the governor’s office told ProPublica, “Governor Sanders looks forward to defending Arkansas’ pro-life laws in court.”
Waldorf’s personal story and deep Arkansas roots seem to have grabbed the attention of people who don’t usually follow abortion policy. Boys she knew in college who she hasn’t talked to in 20 years reached out to say how upset they were to hear about her experience. A pastor she’d known since childhood defended her on Facebook against anti-abortion attacks. Friends who described themselves as “pro-life” have written long messages about how her story has sickened them and how they want the law changed.
Waldorf said she hopes that sharing the details of her trauma may finally make a difference. But it hasn’t stopped her from reliving it all. Fayetteville is small. Barely a day goes by where she doesn’t bump into former co-workers from the hospital — at the grocery store or the coffee shop or school pick-up. Recently, she saw Large a few booths over at a local restaurant.
Each run-in brings it all pouring back. The ultrasounds. The “risk management.” The blood, so much blood.
But also, the state line. The relief she felt crossing it.

#Arkansas #Emily #Waldorf #Died #Denied #Miscarriage #Care #ProPublica